Skip to content
Skip to content 
Table of Contents
Social Work Case Notes Examples & Templates
If you’re a social worker who wants to spend less time writing case notes, you’re in the right place! We’ve got some useful writing tips and best practices to improve your case notes, along with some great case notes examples for social workers.
What Are Case Notes?
Case notes are records of a client’s or patient’s one-on-one meetings with social workers, usually written in chronological order.
Social workers record incidents observed during a visit, their client’s recent history and present circumstances, as well as document their overall progress, goals, and response to various treatments (if undergoing any). Social workers may even interview family members and persons relevant to a given case they’re assessing.
Well-written case notes provide objective descriptions grounded in fact and evidence, and leverage a social worker’s assessments and opinions without bias. They are important for insurance coverage purposes, legal proceedings, and social work continuity as they provide an accurate historical record of treatment.
The social work case notes examples provided here can be used for case management in health and social services in order to track helpline calls, manage beds for clients in shelters, and to track the palliative care of patients in hospices.
What to Include in Case Notes
Before we get to the sample case notes and best practices, let’s take a look at what you should include in your social work case notes.
This guide presents a general overview of what information to include in your case notes. Exactly what must be entered (or left out) is dependent on what is relevant to the service or support you provide.
The Basics
Here’s an outline you can follow to make sure you cover all relevant information:

Who: What is the name and designation of the person submitting the case note?
What: What was done (what services were provided)?
Where: Where did it take place (whether via phone or in-person)?
When: What was the date of service?
Why: What was the reason for interaction and intended goal (whether this is a follow-up meeting, monthly or weekly scheduled meeting, unit inspection, intake or exit meeting)?
Additional Information to Include
Meeting Information and Observations
- Topics discussed during the session
- How the session related to the treatment plan
- How the treatment plan goals and objectives are being met
- Interventions and techniques used during the session and their effectiveness
- Clinical observations along with any facts, theory or research underpinning an assessment
- Tracking of client activities (job pursuits, psychological assessments, etc.)
- Tracking of program/agency monitoring activities (e.g. lab results)
- Evidence that you and the client have discussed your respective legal and ethical responsibilities.
Client/Patient History
- The client’s current strengths and challenges
- Progress or setbacks
- Signs, symptoms and any increase or decrease in the severity of behaviours as they relate to a diagnosis
Follow up information
- Next steps
- Whether or not the next meeting or follow up with the client was scheduled
- Location and time of the next meeting (if scheduled)
- Roles and responsibilities for both the client and yourself (or another case manager) to prepare for your next meeting.
Case Notes Examples for Social Workers
Social work case notes will vary from one organization to another depending on organizational policies, documentation formats, and legal guidelines.
To give you a clear idea of the different styles and formats, we’ll take you through five sample case notes for social workers across different sectors, including shelters, hospices and social service organizations.
But first, let’s look at a few popular documentation formats. Different styles of documentation are used to help social workers organize their notes and prevent key information from being missed. You can choose whichever one works best for your organization.
Here are some common styles:

Sample Case Notes for Social Workers: Health & Social Services
Case Notes Example 1: Rehousing Program
Take a look at this case note example of a home visit from a Family Rapid Re-Housing and Stabilization Program (FRSP). (Note that this does not use a specific documentation style, but follows a clear structure and format and is highly detailed.
Angela Lewis, FRSP case manager, met with Ms. George at her home on 10/24/2019 at 10:00am for her scheduled monthly home visit.
Ms. George was home alone at the time of the home visit as she reported that her children were at school. Ms. George appeared to be in an overall good mood at the time of the visit and was very engaged. Her apartment was free from excess trash and the client’s kitchen was free from excess food debris at the time of the visit.
There also appeared to be no maintenance concerns in the unit. During the home visit with Ms. George today, the writer completed and reviewed the Housing and Participation Assessment Report (HPAR) and also assisted Ms. George with completing her monthly budget.
The writer engaged Ms. George in a conversation about her progress with her goal of increasing her income. Ms. George shared that she completed about three job applications this month which included: Starbucks, Target and Marshalls. She reported that she has not yet heard back from Marshalls or Target, but shared that Starbucks contacted her for an interview which is scheduled for November 5th 2019 at 2pm.
Ms. George confirmed that she will attend her job interview with Starbucks at 2pm on 11/5/2019 and also reported that she will continue to use Indeed.com as her method of searching and applying for jobs. In addition to continuing her job search, the writer suggested that Ms. George also contact Marshalls and Target in effort to follow up on the status of her applications in which Ms. George agreed to do so.
Ms. George shared her goal to apply for a total of 6 jobs during the month of November. Ms. George is scheduled for a follow up phone call with the writer on 11/15/2019 at 11am regarding her progress with her job search.
Case Notes Example 2: Welfare Visit
This is another case notes example of a home visit, written in the S.O.A.P. documentation style.
S = Strengths
I met with Mrs. Diaz on xx/xx/xx. Despite her financial and health concerns and her reported sadness, she has followed through with most previously agreed upon tasks. She also reached out to her children this past week, which resulted in her receiving a nice visit from her son and his family. She said that she felt in slightly better spirits because of it.
O = Objective Account
Mrs. Diaz reported that she went to the food bank and has enough food to last until her next social security check arrives next week.
With my assistance, Mrs. Diaz completed an application for food stamps. We also made an appointment for her at the food stamps office on Friday and I provided her with a Metro Card to get to and from her appointment. She stated that she did not call the Community Health Center to make a medical appointment as planned.
When I asked her why she didn’t follow through with this, she said she is uncomfortable attending a community health center and that she is fearful of what the doctor might tell her. This writer also provided Mrs. Diaz with a referral to Agency T for financial counselling and tax preparation. This writer scheduled an appointment at Agency T on xx/xx/xx.
A = Assessment
Ms. Diaz has followed up on all tasks agreed upon with the exception of making a medical appointment and says she is feeling more hopeful.
P = Plan
- Ms. Diaz is looking forward to attending her first yoga/movement class at the senior center tomorrow.
- She will attend her intake appointment to complete the food stamps application process on Friday.
- She will attend her appointment with the financial counsellor on xx/xx/xx. The plan to go to the community health centre was revised and Mrs. Diaz was given a list of private M.D.’s that accept Medicare. Mrs. Diaz will make an appointment with one of the doctors this week.
- This writer will check in with Mrs. Diaz via phone every Friday for the next month and we will meet again in person one month from today.
Sample Case Notes for Social Workers: Medical & Palliative Care
Case Notes Example 1: Medical Checkup
S = Strengths
Client reported difficulties in keeping appointments with providers including this case manager, ADAP, and the doctor. Client expressed concern with memory issues and transportation challenges.
O = Objective Account
Client was polite and joking throughout the meeting. He was neatly dressed, well spoken but had to stop to think about what he was saying as he had trouble staying focused.
A = Assessment
Client is at risk of being non-adherent to medications and other appointments. Client needs reminders to assist with keeping appointments, a pillbox to help with medication adherence and help with transportation.
P = Plan
Provide client with a pillbox and have a nurse in the clinic assist in setting it up. Provide client bus tokens to assist in getting to appointments. Call client 24 hours prior to visit with case managers as a reminder.
Case Notes Example 2: Palliative Care
50 hours after initial admission visit Mrs. Violet is in visible pain upon entering the room. She is miserable. Moaning and tossing and turning in the bed. She has been taking her Lortab 10/500 as directed, taking 1 every 8 hours. The Roxanol® has not been filled. The patient’s daughter is afraid that she will “kill“ her mother with the morphine.
Mrs. Violet is nauseated, unable to tolerate even water. She has not had any of the meds from the comfort kit. Her daughter has not wanted to “bother” the Hospice staff for instructions on how to use the “Comfort Kit” (preordered medications to assist with s/sx during crisis). Pollyanna received instructions initially but did not think she would need it.
There has been no bowel movement since prior to her hospitalisation 7 days ago now. You now suspect some sort of intestinal obstruction. The patient is adamant that she does not want surgery. She does agree that in the hospital that she might be able to get more comfortable with the aggressive pain management (IV meds, PCA pump possibly).
Mrs. Violet’s daughter states that as long as her mother can make her own decisions that the family will abide by them. Decision is made to transfer to GIP for Pain and intractable nausea symptom control.
Case Notes Example 3: Care Plan Visit (DAP Format)
(Data) Clinic-visit with client to complete and update care plan. Client spent most of the visit talking about her medications. She mentioned that she gets sick often and suffers from nausea from time to time for no apparent reason. She said she has tried to follow the directions given by the doctor, but is concerned about the recent weight loss she has had and wonders if it is due to the medications.
(Assessment) Client fidgeted, talked fast, and seemed stressed over her medical condition. During the visit she spoke little about her family life, she seemed to be more preoccupied with having her meds changed and getting past the nausea. Not much improvement from her last visit.
(Plan) Will follow up with client to ensure she relates info to her doctor during her next visit and refer for adherence counselling until client feels better. Continue to work with client on adherence.
Creating & Entering Case Notes
Creating and entering new case notes is something caseworkers need to do on a regular basis, so it should be really easy and straightforward. Using web-based case notes software like Sumac Case Portal can help.
With Sumac Case Portal, caseworkers to enter case notes, and manage clients and meetings from a mobile phone, tablet, or laptop. Just find find the client, select case manager, program, and enter the notes. When the case notes are saved, they are automatically attached to the client’s record in chronological order.
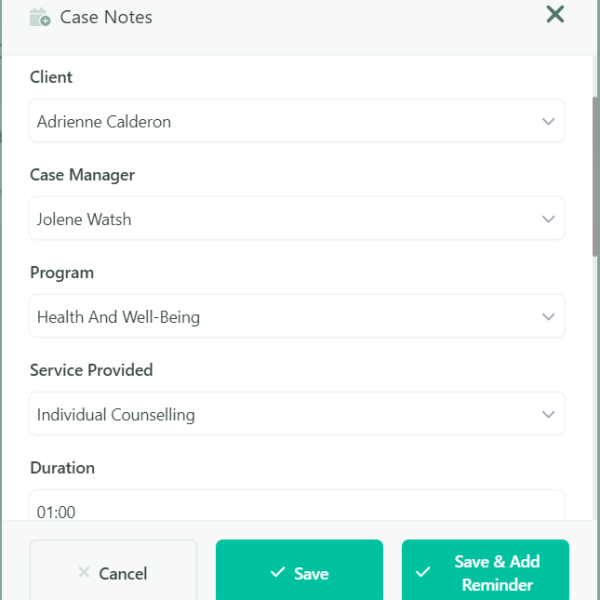
If you’re using Sumac nonprofit case management software in conjunction with Case Portal, your case notes template will be configured for the exact needs of your social service organization, so entering case notes is really easy

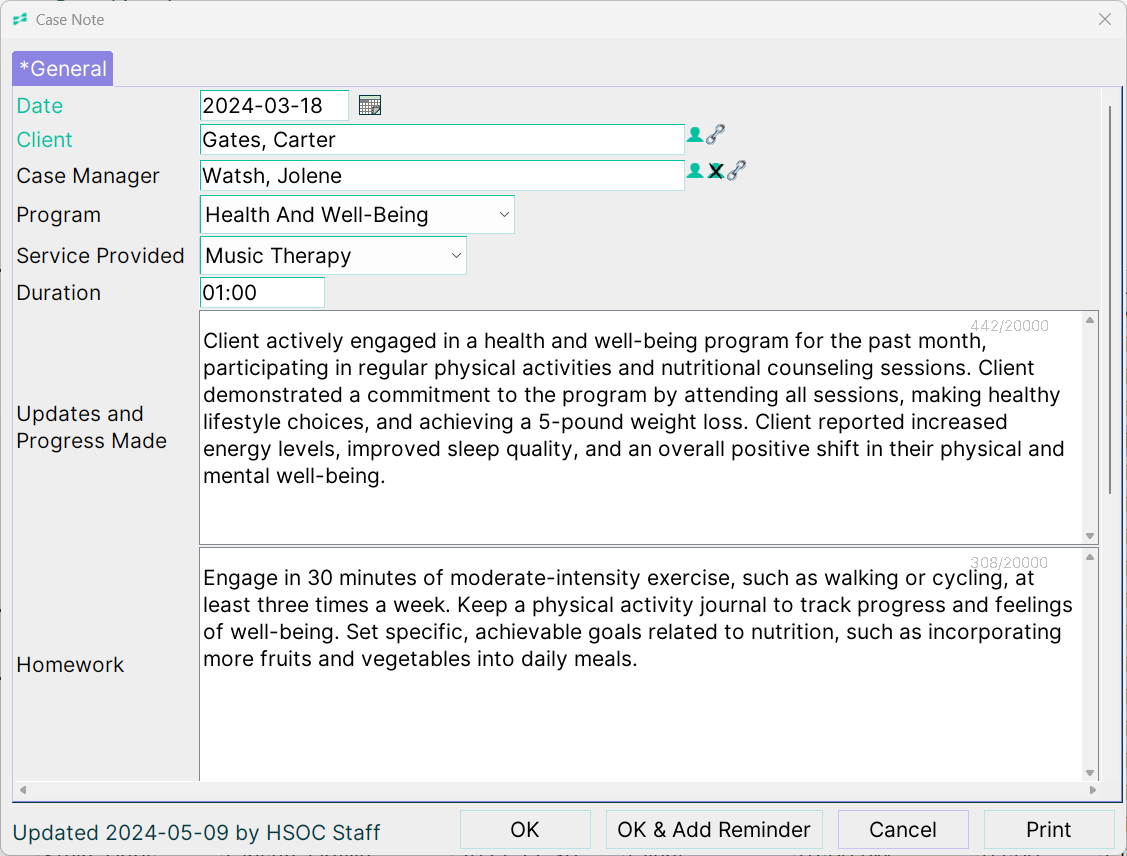
Case Notes Examples: Health & Social Services
For Health & Social Services, your case notes template will be configured with your services in a drop down menu, along with other configurations you need.
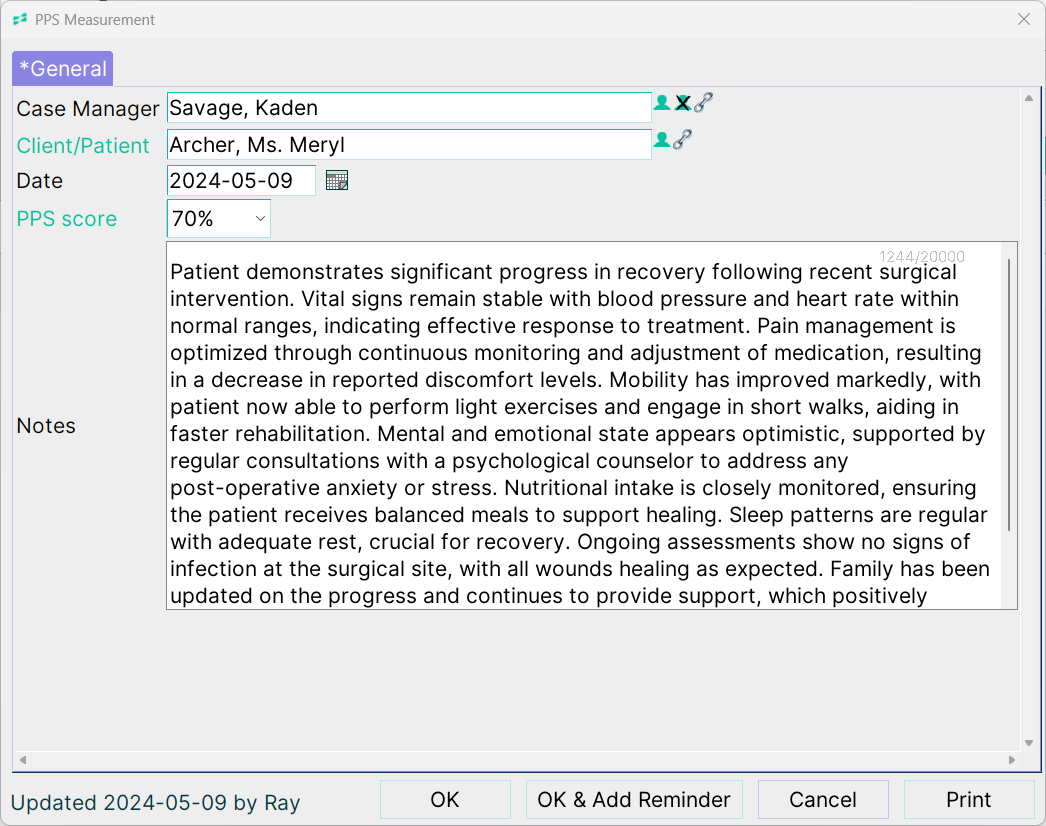
Case Notes Examples: Hospice & Palliative Care
For Palliative Care & Hospice, your case notes template will be configured with a drop down so you can record PPS score, along with other configurations you need.
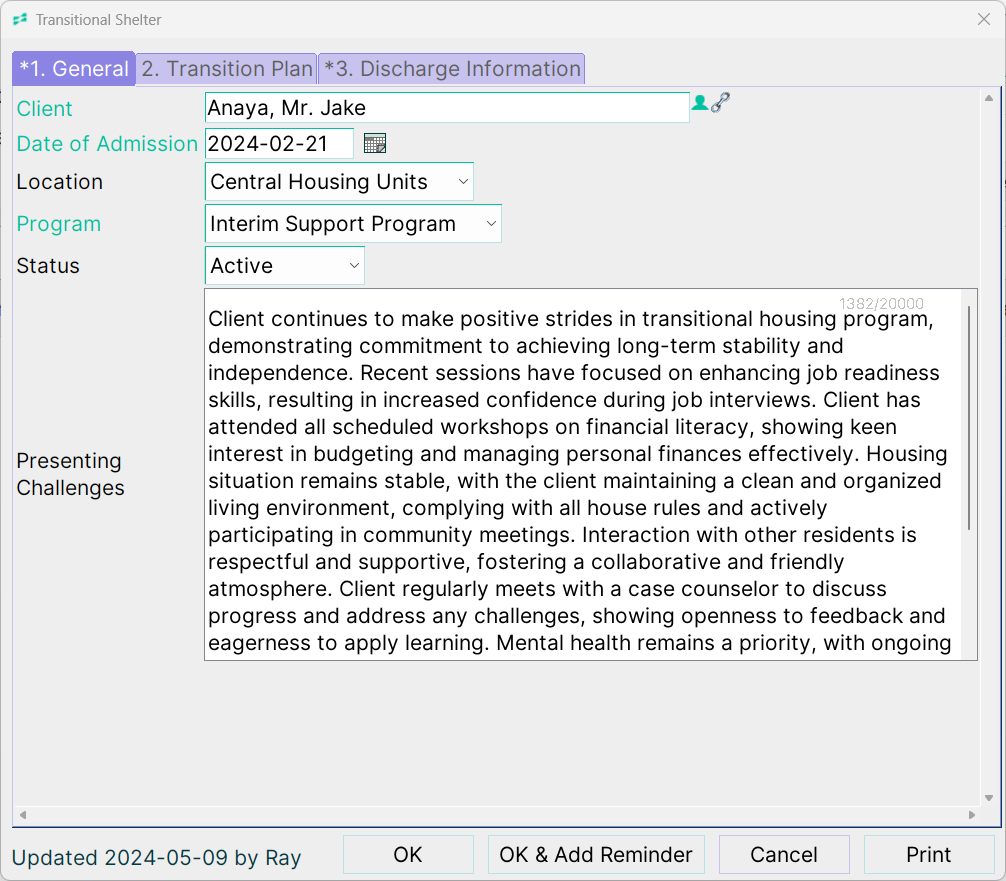
Case Notes Examples: Shelter & Transitional Housing Software
For Shelter & Transitional Housing, your case notes template will be configured with a drop down to indicate the reason for contact, along with other configurations you need.
Best Practices for Writing Case Notes
Let’s take a look at some best practices and writing tips to help you create timely and accurate case notes.
1. Write Clearly and Accurately - Sticking to the Facts
When writing case notes make sure you are as clear, concise, and factual as possible. Your notes should be easy to read, and not use overly complicated sentences. Besides your observations, you should also document any legally relevant information, especially if any aspect of treatment presents a liability to you or the client.
A good way of keeping your notes as detailed and accurate as possible is to record them in a timely manner, either soon after your meeting or the next day. If you are pressed for time, summarise the meeting and note a few key points immediately after. You can then write out a more detailed version of your case notes when you have the time. This way, you won’t forget important observations that could be relevant to a client’s treatment.
Once you have your case notes written down, review the information to ensure that it is up to date, accurate and grammatically correct.
Litmus Test for a Good Case Note
- When you are unable to be present, a colleague can open the record and easily figure out the next step to help the client achieve their goals.
- If your client read the note, they would feel respected and would agree with your objective account of the interaction.
2. Don’t Use Abbreviations
Social workers often use abbreviations and jargon in their day-to-day lives, and it’s very tempting to continue to do this in your case notes, as it would definitely speed things up. But if you want someone else to be able to read your notes and understand everything you’ve included, you should avoid using jargon.
Case notes are sometimes read by people outside your sector, often by judges and others in the legal profession. If your notes aren’t legible and an emergency arises, this can become a liability issue. So avoid using acronyms, abbreviations, or any kind of shorthand.
3. Avoid Value Judgements
Good sample case notes for social workers are free of value judgements. They include observations about a client’s appearance or behaviour without judgement, and are as objective as possible.
Take a look at this social work case notes example text:
“[Client] was dressed very shabbily and smelled bad.”
This text is subjective and provides little value. A note indicating that a client has stopped wearing clean clothing or that their clothing is looking progressively more damaged, is a better way to present this information.
One way of ensuring your case notes remain free of derogatory and emotive language, or value judgements is to think about how it would make your client or patient feel to have these notes read out to them. If it wouldn’t sit well, you’re very likely making a value judgement rather than stating facts or observations.
4. Protect Your Client’s Privacy
When writing case notes, it’s important to keep a client’s privacy in mind while documenting relevant information for your treatment goals.
It’s a good idea to only include detailed information relevant to the provision of a support or service to which your client has consented. For example, rather than detailing every aspect of a fight with their spouse, you might only note that the client had a fight with their spouse, or that it follows an ongoing pattern.
Here are a few topics with sensitive information you should protect:
- Information regarding legal status and criminal records
- Substance Abuse
- Domestic Violence
- Health (Physical or Mental)
To protect your client’s privacy regarding these matters, our sample case notes for social work include the following statement:
“The client reported that he or she is currently involved in the legal system/ seeking care or treatment from a doctor for a medical condition/has been connected to domestic violence resources.”
5. Separate Observation From Opinion
It’s important to separate your opinion from your observation. Engage your five senses when describing the meeting. State clearly what you saw, heard, touched, smelt, or even tasted.
Back up facts and observations with evidence and clearly distinguish between this and your personal opinion. Opinions can be important when making decisions about treatment options or assessing a situation, but they must not be written as facts.
Take a look at this social work case notes example text:
“Patient seemed anxious”
This is an opinion that provides little value. Instead say something like: “Patient expressed fears about the future, was shaking, and said she was having panic attacks.” This is factual, well-observed, and provides relevant details without including an opinion.
6. Customise Your Case Notes for Your Organization
If case workers need to write a lot of case notes, you can streamline the process and make it better fir your programs and services with case note templates that are customised for your organization.
Let;’s face it, no two social service organizations are alike and different organizations will need to capture different information. Having a case notes template that fits your organization will help social workers do their job better and more efficiently, and lead to more valuable case note recordings overall.
If you’re using Sumac case management software, this case notes configuration is included for different types of organizations like health and social services, shelters, helplines and hospices, so you can choose a template most relevant to your type of service, and even customize it further do it fist your nonprofit’s exact needs.
7. Schedule Time for Case Notes
It’s a good idea to schedule 10-15 minutes either directly after each session to draft your case notes. This will help you record notes while the memory is still fresh, and you’ll never have to deal with a large pile of case notes at the end of a busy week. You can then spend time later writing them up in more detail.
Writing notes directly after a session also gives you time to reflect on the session and make notes for next steps and follow ups.
While you should make notes after a session, reviewing case notes before a new session can also be helpful. This will set the context for you and remind you of key pieces of information or conversations in earlier sessions. It can also help guide the session, and ensure both you and your client stay focused on treatment goals.
8. Keep Your Data Secure
Case notes contain highly sensitive information about your clients, including their symptoms, fears, conflicts and treatment goals, as well as their diagnosis and treatment history. It’s for this reason they’re given the same protection as medical records.
Confidential information such as this is protected under the Health Insurance Portability and Accountability Act (HIPAA) in the US and the Personal Information Protection and Electronic Documents Act (PIPEDA) in Canada.
Nonprofits that don’t comply could face thousands – if not millions – of dollars in fines. The safest way to store case notes is to keep them in a password-protected, encrypted cloud storage system with limited access. For example, you should select a case management software like Sumac’s which is HIPAA and PIPEDA compliant and limits access to case notes to only select staff.
Physical security is also important, especially if you store case notes manually. Lock rooms with treatment or case notes in password-protect computers.
9. Learn About Your Legal Responsibilities
Case notes may be subject to a range of legislative processes and requirements during and after the conclusion of the relationship. Depending on where you live, your country, state, or province may have different rules regarding case notes and legal requirements. It is your responsibility to be aware of them before you begin recording your interactions with clients.
For example, if someone indicates a desire to harm themselves and you are legally required to notify a third party, indicate the nature of the threat, and note who you notified and how, in your case notes. This will also serve as a legal record of events.
You should not only be familiar with the general guidelines of case note management but also how these requirements are implemented within your organization.
10. Use Technology to Manage Case Notes
Using case management software can help you create case notes more efficiently, eases the administrative burden on social workers with heavy caseloads, and enhances the quality of service you provide.
Here are a few ways technology can help:
- Eliminate paper: With case management software, all records are filed and stored online or on your computer, eliminating the need to handle and store paper records. Typed entries also ensure that records are easily readable.
- Access documents securely: Software can be password-protected and encrypted to ensure only those with access can obtain your documents. It’s much more difficult to access patient records when stored in HIPAA and PIPEDA compliant software like Sumac.
- Streamline patient registry: Online forms can be embedded on your website, so clients can register and complete a case intake questionnaire directly on your website. With seamless CRM integration, data is updated automatically, so there’s less effort and less errors.
- Find documents easily: Digital storage means that your case notes are well-organized and easily searchable. With Sumac case management software each case note is connected to a client’s record and date stamped, so you can view a chronological history of all notes and easily locate specific ones.
Conclusion
Writing accurate and well-informed case notes is a key skill all social workers need to cultivate.
Detailed, factual notes are an important practice tool that help govern treatment decisions, accurately measure outcomes, and provide an important historical record of a client’s behaviour and symptoms. They can even help improve treatment outcomes and expedite a client’s overall progress.
Try using a case management software to help you record accurate and detailed case notes. This will ensure they are not only secure, but you’ll also be able to easily share them with doctors and other authorized social workers who require this information.